Division of Infectious Diseases
Antimicrobial Resistance is a Global Problem: Notes from the World Health Summit
From the World Health Summit, Berlin: Panel on Antimicrobial Resistance (AMR), October 27, 2019. The 2019 World Health Summit (#WHS2019) opened with a panel discussion about the accelerating problem of global antimicrobial resistance (AMR). Dr. Peter Beyer, an intellectual property law expert working with the WHO on global health applications, led a panel of international […]
Nov 26, 2019

Nebraska Medicine receives IDSA Antimicrobial Stewardship Center of Excellence Designation
In 2018, the Infectious Diseases Society of America (IDSA) began recognizing “Antimicrobial Stewardship Centers of Excellence” at hospitals that meet or exceed best practice standards. We are pleased to announce that Nebraska Medicine has recently been designated as an Antimicrobial Stewardship Center of Excellence effective October 2019. As we celebrate #AntibioticAwarenessWeek for 2019, we are reminded […]
Nov 22, 2019
Antimicrobial Stewardship efforts in the state of Nebraska
Content provided courtesy Dr. Salman Ashraf: Associate Medical Director, Nebraska Antimicrobial Stewardship Assessment and Promotion Program (ASAP) & Medical Director, Nebraska Infection Control Assessment and Promotion Program (ICAP) CDC’s most recent (2019) report on Antibiotic Resistance Threats in the United States describes 2.8 million infections due to antibiotic resistant organisms in the US resulting in over […]
Nov 21, 2019
#BeAntibioticsAware in the Community Hospital Setting
Bellevue Medical Center (BMC) is a community hospital campus of Nebraska Medicine. In 2017, our Nebraska Medicine Antimicrobial Stewardship Program expanded to include BMC with the expansion of our ASP expertise at our main campus. Danny Schroeder, a pharmacist at BMC, was recruited to lead the stewardship activities on that campus, with expertise provided by […]
Nov 20, 2019

Celebrating Antibiotic Awareness Week in Nebraska!
Antibiotic Awareness Week Proclamation Signing Ceremony CDC has designated November 18 to 24 as US Antibiotic Awareness Week. Antibiotic Awareness Week is an annual observance in the United States and around the world to promote the importance of using antibiotic appropriately as a mean to minimize unwanted effects from antibiotic therapy (e.g., adverse reactions, Clostridioides […]
Nov 18, 2019

Antibiotic Awareness Week Is Coming! How Will YOU Raise Awareness??
CDC has designated November 18-22, 2019 as US Antibiotic Awareness Week! We are joining the CDC and many organizations around the world recognizing and promoting awareness for appropriate antibiotic use. During #AntibioticAwarenessWeek, collaborative blog posts from UNMC ID/ASP and Nebraska ASAP will be published between November 18 and 22. Check out these videos supporting the Antibiotic […]
Nov 17, 2019
Are you ever involved with prescribing antibiotics in the hospital? We want to hear from you!
The Nebraska Medicine Antimicrobial Stewardship Program (ASP) invites you to participate in a research survey entitled: Use of Oral Antibiotic Therapy (OAT) for Definitive Treatment of Uncomplicated Bloodstream Infections (uBSIs): Opportunities for Antimicrobial Stewardship. There are several studies describing successful use of oral antibiotics to treat bloodstream infections, but are clinicians actually using oral antibiotics […]
Nov 14, 2019

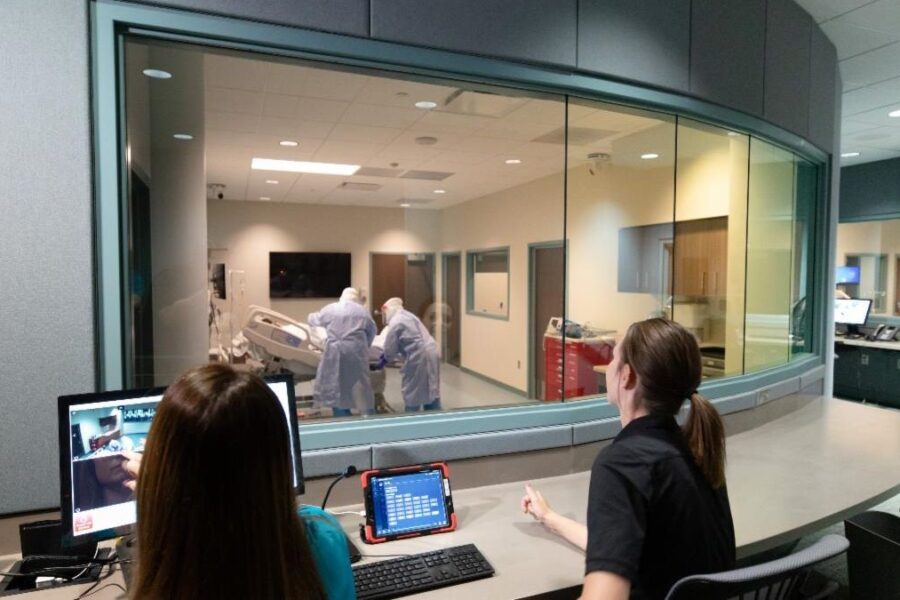
UNMC Global Center for Health Security opens new National Quarantine Center
The UNMC Global Center for Health Security (GCHS) has expanded its capability and national role in quarantine care through the establishment of a 20-bed quarantine unit located within the Davis Global Center for Advanced Inter-professional Learning. The National Quarantine Center, funded in October 2016 by a $20 million dollar award from the Assistant Secretary of […]
Nov 12, 2019
EMR Order Set Speeds Time to Antibiotic Treatment in Musculoskeletal Infections
Dr. Angela Hewlett spends her time at UNMC not only studying Ebola but also working to prevent and manage musculoskeletal infections. In addition to publishing this year’s update on “What’s New in Musculoskeletal Infection,” she collaborated with orthopedic surgeons, trauma surgeons, and emergency physicians to design and implement a new order set in the UNMC […]
Nov 5, 2019
Medical Student Musings from #UNMCHIV2019
This year, the UNMC HIV Update for Care Providers and Educators on October 10, 2019 brought approximately 100 attendees to Omaha again to learn about new drugs, management approaches, and patient experiences with HIV. The CME conference was funded by the Nebraska AIDS Education & Training Center (AETC), [a local partner of the Midwest AETC], and […]
Oct 30, 2019

Recent Comments