Division of Infectious Diseases
Seeking a Full-time Physician to Join UNMC’s HIV Program
The Division of Infectious Diseases at the University of Nebraska Medical Center in Omaha, NE is looking to add an ID physician to join our well-established HIV team recognized for providing expert care locally, regionally, and nationally. As the largest provider of care to patients living with HIV in the Omaha area, the HIV clinic […]
Jan 19, 2022

Nebraska Tropical Medicine Course
Learn more about the Nebraska Tropical medicine course. This familiarization and refresher course has an expanding list of activities for physicians, nurses, and other allied health professionals seeking to better expand or renew their awareness of tropical medicine issues.
Dec 20, 2021

Learn more about our open Community ID physician position!
Content provided by Dr. Starlin Our community infectious diseases team aims to provide service to patients outside of main University of Nebraska Medial Center (UNMC) campus. It is one of the few fully dedicated Academic Community Infectious Disease services in the country and we are proud to embrace Nebraska Medicine’s (NMC) and UNMC’s vision and […]
Nov 23, 2021

Antibiotic Awareness Week Publication Alert: Confronting antimicrobial resistance beyond the COVID-19 pandemic
Antibiotic Awareness Week 2021,”an annual observance that raises awareness of the threat of antibiotic resistance and the importance of appropriate antibiotic use” runs this year from November 18-24 2021. This is a global campaign with messaging from the CDC and the WHO calling on all of us to not only Be Antibiotics Aware, but to actively engage in activities to reduce the spread of antimicrobial resistance. To kick off #USAAW21 and #WAAW21, we share this #ThrowbackThursday publication from September 2020: Confronting antimicrobial resistance beyond the COVID-19 pandemic and the 2020 US election.
Nov 18, 2021

UNMC ID Antimicrobial Stewardship Pharmacists celebrated with Acute Care Pharmacist of the Year and Rising Star Pharmacist Awards
Thirty-three acute care pharmacists received heartfelt nominations from sixty-five peers and colleagues for Pharmacist of the Year 2021. This year, two awards were given – the Acute Care Pharmacist of the Year Award, and the Rising Star Pharmacist Award: both awardees came from the UNMC ID division.
Nov 15, 2021
Round 2: IDWeek 2021 “Ryder’s Review”
Once again this year, Dr. Ryder felt quite fortunate to attend this conference as part of his fellowship training, as the emphasis on fellow education at UNMC is clear. He shares his IDWeek2021 experience here.
Nov 9, 2021

COVID-19 vaccines at the Specialty Care Center
Since mid-August 2021, the Nebraska Medicine Specialty Care Center (SCC) has been busy administering Pfizer BioNTech COVID-19 vaccine to patients at the clinic. Many of these patients were previously hesitant about receiving COVID-19 vaccines elsewhere in the community, but had expressed willingness to complete it at the SCC.
Nov 2, 2021
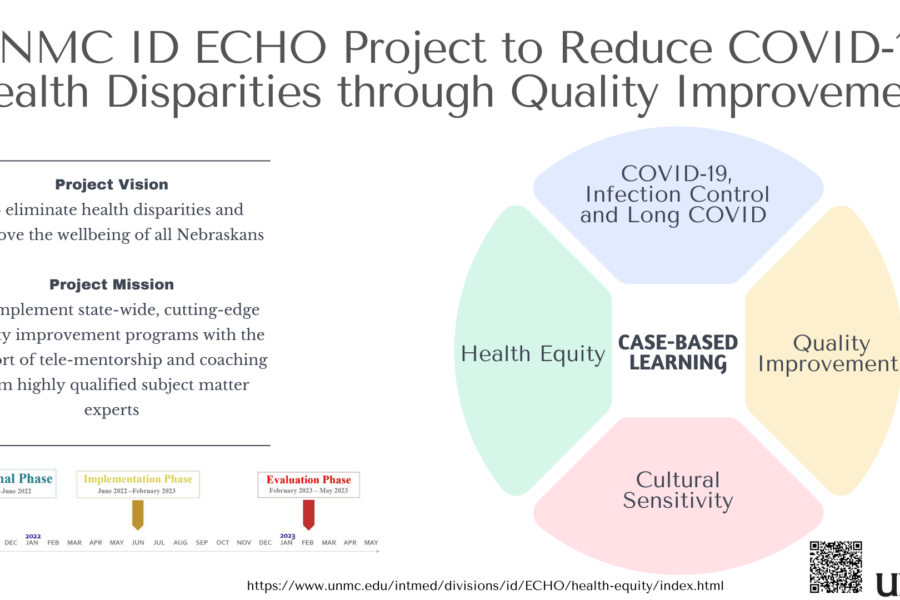
Introducing a new Nebraska DHHS funded UNMC ID ECHO Educational Series
Introducing a newly launched educational initiative, the UNMC ID Health equity and Quality Improvement ECHO Project. The goal of the program is to achieve health equity, address COVID-19 disparities, and improve the health of all Nebraskans using a quality improvement approach. The course is being offered at no cost to the learners through the University […]
Oct 26, 2021
We appreciate our ID Pharmacists
We LOVE our UNMC ID Pharmacists! Today marks the end of National Pharmacy Week and we want to share our appreciation and thanks for the hard work and invaluable contributions of our pharmacists at UNMC ID. Our pharmacists are exceptional clinicians giving us the clinical advice we need on antimicrobials and drug interactions. They are […]
Oct 22, 2021

Publication Alert: Structural Vulnerability among Patients with HIV and SARS-CoV-2 Co-Infection
Publication Alert: Structural Vulnerability among Patients with HIV and SARS-CoV-2 Co-Infection. This content was provided by Natasha Hongsermeier-Graves, MD/MPH student at UNMC College of Medicine/Harvard School of Public Health. She led a recently published study, collaborating with another UNMC medical student Rohan Khazanchi, and UNMC ID faculty Drs. Jasmine Marcelin and Nada Fadul.
Oct 19, 2021

Recent Comments