Division of Infectious Diseases
At the end of 2018, we remember and respect Influenza, 100 years after the great pandemic
The Mother of All Pandemics In the 1918-1919 calendar year, the world experienced the worst influenza pandemic in modern times. Coming on the heels of WWI, the H1N1 pandemic occurred in three waves – in the spring of 1918, fall 1918 and spring 1919. Estimates suggest that the pandemic infected a third of the world’s […]
Dec 26, 2018

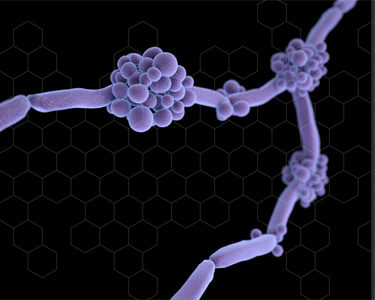
Pharm To Exam Table – Candida glabrata Urinary Tract Infections
The following is a clinical review written by Allison Graner, UNMC College of Pharmacy PharmD candidate 2019, and supervised by Scott Bergman PharmD FIDSA, Clinical Pharmacy Coordinator of Nebraska Medicine Antimicrobial Stewardship Program What is the appropriate treatment for urinary tract infection caused by Candida glabrata? Infections caused by the fungus known as Candida, the […]
Dec 21, 2018
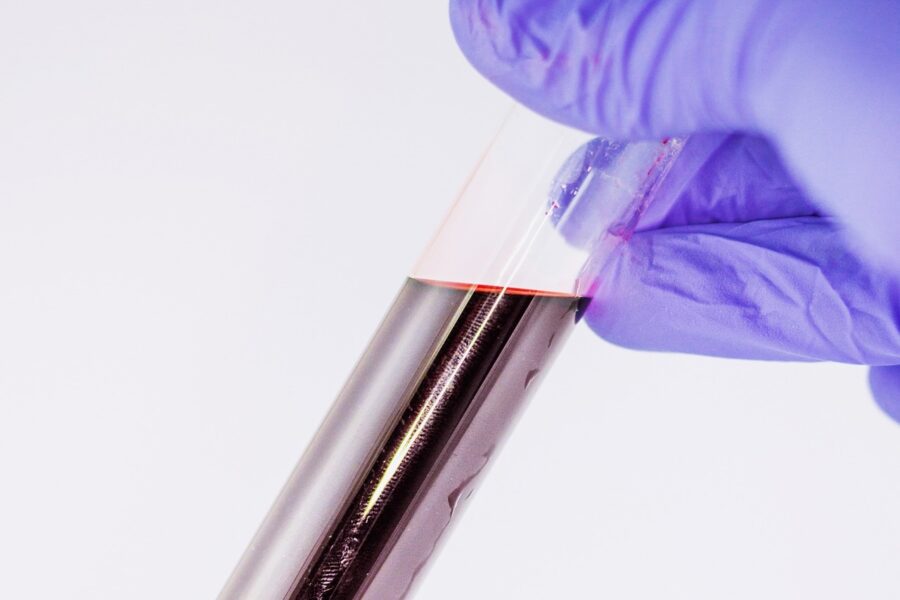
Bacteriocidal versus Bacteriostatic: What Makes the Biggest Difference in VRE Bloodstream Infection?
An October 2018 publication in Critical Care Medicine by Chuang et al details a prospective study of adults in Taiwan, between 2010 -2015, aimed to assess all-cause mortality and rate of bloodstream clearance among patients with vancomycin-resistant enterococci (VRE) treated with daptomycin (bacteriocidal) versus linezolid(bacteriostatic). Patients were treated with conventional daptomycin (6 to < 9 mg/kg […]
Dec 19, 2018
Saving SIRS? Discernment of Sepsis from Non-Infectious Syndromes in the ED
Upon patients’ arrival to the emergency department (ED), determining whether they do or do not have sepsis is difficult. Because of this, many patients receiving antibiotics ultimately are found to have a noninfectious cause of their syndrome. In order to try and improve detection of sepsis in the ED, Mearelli et al. completed a multicenter […]
Dec 10, 2018

Skin Deep: A Closer Look at Treatment of Skin and Soft Tissue Infections
Current guidelines for management of Skin/Soft Tissue Infections (SSTIs) were published in 20141. Nevertheless, management of SSTIs is variable, likely driven by the fact that culture data is often unavailable to direct clinical decision making. Treatment variability results in inappropriate antimicrobial use, highlighting the need for antimicrobial stewardship. Consequently, management of SSTIs is one area […]
Dec 3, 2018

Top 10 Things We Are Thankful for in ID – Letterman Style
Life is better with gratitude. Today, whether or not you celebrate Thanksgiving, we want to continue to show our gratitude and thankfulness to be able to help diagnose, prevent, treat, cure and even advance, the science of medicine. Now, let’s have a little fun! We are grateful for: 10. Hand washing with those cute seasonal […]
Nov 22, 2018

Earrings In Healthcare Workers: Friend or Foe?
Ear piercing among people, including healthcare workers, is a common trend. Katsuse et al, attempted to make a correlation between ear piercings and healthcare-associated infections. In order to prove this relationship, researchers sampled the earlobes and fingers of 200 nurses working at a university hospital. 128 of those nurses had pierced earlobes and 72 of […]
Nov 20, 2018

UNMC Infectious Diseases Fellows are Antibiotics Aware
The following was written by Dr. Raj Karnatak, 2nd year ID fellow at UNMC; a reflection of his current Antimicrobial Stewardship/Infection Control rotation: The UNMC Infectious Diseases fellowship antimicrobial stewardship and infection control rotation provides robust training for fellows in both antimicrobial stewardship and infection control. Training is well designed with education in all the […]
Nov 16, 2018
How Nebraska ASAP is Making Everyone Antibiotic Aware
The following was written by Dr. Salman Ashraf, co-Medical Director of the Nebraska Antimicrobial Stewardship Assessment & Promotion Program (ASAP): Antibiotic Resistance is one of the most urgent threats to the public health. Overuse and misuse of antibiotics allows the development of antibiotic-resistant bacteria. Unfortunately, a significant proportion of antibiotic use in various healthcare settings […]
Nov 15, 2018
Nebraska Medicine is Proud to #BeAntibioticsAware
Our Antimicrobial Stewardship Program (ASP) at Nebraska Medicine has been in place since 2004. Over the years our program has changed and improved sought to expand and improve its approach with the goal of providing extraordinary care to our patients. Rather than an overly restrictive practice, our program has we have emphasized constant regular communication […]
Nov 14, 2018
Recent Comments