Division of Infectious Diseases
COVID-19 vaccines at the Specialty Care Center
Since mid-August 2021, the Nebraska Medicine Specialty Care Center (SCC) has been busy administering Pfizer BioNTech COVID-19 vaccine to patients at the clinic. Many of these patients were previously hesitant about receiving COVID-19 vaccines elsewhere in the community, but had expressed willingness to complete it at the SCC.
Nov 2, 2021
Introducing a new Nebraska DHHS funded UNMC ID ECHO Educational Series
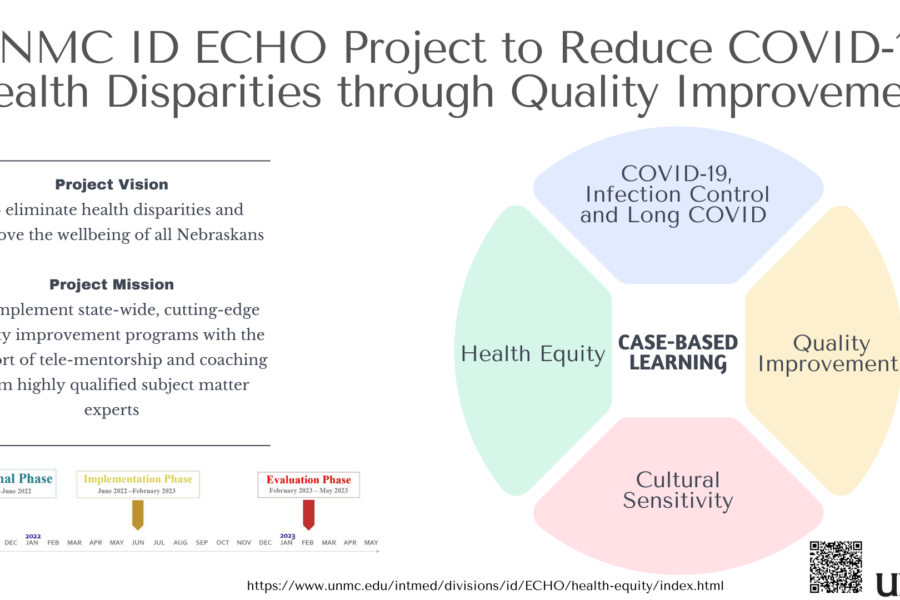
Introducing a newly launched educational initiative, the UNMC ID Health equity and Quality Improvement ECHO Project. The goal of the program is to achieve health equity, address COVID-19 disparities, and improve the health of all Nebraskans using a quality improvement approach. The course is being offered at no cost to the learners through the University […]
Oct 26, 2021
We appreciate our ID Pharmacists
We LOVE our UNMC ID Pharmacists! Today marks the end of National Pharmacy Week and we want to share our appreciation and thanks for the hard work and invaluable contributions of our pharmacists at UNMC ID. Our pharmacists are exceptional clinicians giving us the clinical advice we need on antimicrobials and drug interactions. They are […]
Oct 22, 2021

Publication Alert: Structural Vulnerability among Patients with HIV and SARS-CoV-2 Co-Infection
Publication Alert: Structural Vulnerability among Patients with HIV and SARS-CoV-2 Co-Infection. This content was provided by Natasha Hongsermeier-Graves, MD/MPH student at UNMC College of Medicine/Harvard School of Public Health. She led a recently published study, collaborating with another UNMC medical student Rohan Khazanchi, and UNMC ID faculty Drs. Jasmine Marcelin and Nada Fadul.
Oct 19, 2021

Publication Alert : “Moment vs Movement: Mission-Based Tweeting for Physician Advocacy”
Drs. Kelly Cawcutt & Jasmine Marcelin have served as Co-Directors for Digital Innovation & Social Media Strategy for UNMC ID for several years, and continue to strive to advance communication, amplification, advocacy and education from the Infectious Diseases Division at UNMC, and in the field of Infectious Diseases, as a whole. With that, they […]
Oct 12, 2021
Looking forward to meeting you at the #IDWeek2021 Virtual Career Fair!
Looking for your first position out of fellowship, or your next fulfilling position in your journey? The UNMC ID Division is a robust group comprised of 27 ID physicians, advanced practice providers, pharmacists, and clinical and research support staff. Looking forward to meeting you at the #IDWeek2021 Virtual Career Fair on 10/14/21!
Oct 11, 2021
Welcoming our new Infectious Diseases Pharmacy Resident: Jeremy Tigh PharmD
We are excited to welcome Jeremy Tigh PharmD as a new PGY-2 in our ID Pharmacy Residency Program! He’s the third ID Pharmacy resident we have had and a fantastic addition to our team! Read on to learn a little more about him…
Oct 5, 2021

UNMC ID @IDWeek2021 – Where To Find Us
It is that time of year again, the fresh transition into fall, and for the Infectious Diseases world, the growing excitement for IDWeek. This year, UNMC ID will again be active at throughout the conference. Where can you find us? First, follow us on Twitter @UNMC_ID throughout the conference! Second, we have faculty who will […]
Sep 28, 2021
Hot Topics in Healthcare – HAIs and Infection Prevention Post-Pandemic
Post written by Dr. Kelly Cawcutt & originally posted at https://www.cloroxpro.com/blog/hot-topics-in-healthcare-hais-infection-prevention-post-pandemic/ The COVID-19 pandemic has brought unprecedented changes to healthcare throughout the world. Fraught with high volumes of patients and paucity of resources and testing, combined with personal protective equipment (PPE) and staffing shortages the past year has taught the healthcare community lasting lessons in resilience. The […]
Sep 13, 2021
High-level Review: Updated STI Guidelines Part 2
In July 2021 the Center for Disease Control and Prevention (CDC) released their sexually transmitted infections (STI) treatment guideline, an update from 2015.1 Below, senior ID fellow Dr. Jonathan Ryder highlights significant (but by no means comprehensive) changes in this new guideline that can be incorporated into clinical practice and some of the evidence supporting these changes. Part 2 – Bacterial Vaginosis, Trichomonas, Pelvic Inflammatory Disease
Sep 7, 2021

Recent Comments