
In this article review we learn about the impact of a large-scale, multi-institutional Antimicrobial Stewardship Intervention on significantly reducing the overall use of ertapenem without subsequent downstream effect on carbapenem-resistant Enterobacteriaceae (CRE) non-susceptibility patterns.
Delgado A, Gawrys GW, Duhon BM, Lee GC (2017). Impact of an Antimicrobial Stewardship Initiative on Ertapenem Use and Carbapenem Susceptibilities at Four Community Hospitals. J Infect Dis Ther 5: 341. doi:10.4172/2332-0877.1000341
Ertapenem has no activity against Pseudomonas spp. isolates, and although there is a theoretical risk of increasing carbapenem resistant Pseudomonas spp. isolates with ertapenem use, clinical studies have demonstrated that this is not the case. Nevertheless, ertapenem use can potentially select for CRE, and there remains clinical value in minimizing its use.
The authors conducted a retrospective pre-post quality improvement study designed to reduce ertapenem usage, hoping to also demonstrate an effect in the prevalence of resistant Pseudomonas spp. and Enterobacteriaceae as a result of this intervention. The multifaceted stewardship intervention was largely educational, but was supported by modification of electronic orders and providing audit-feedback opportunities to high frequency prescribers. They also included as a counter measure, evaluation of use of other alternative antimicrobials.
Copyright: © 2017 Delgado A, et al. Click to enlarge
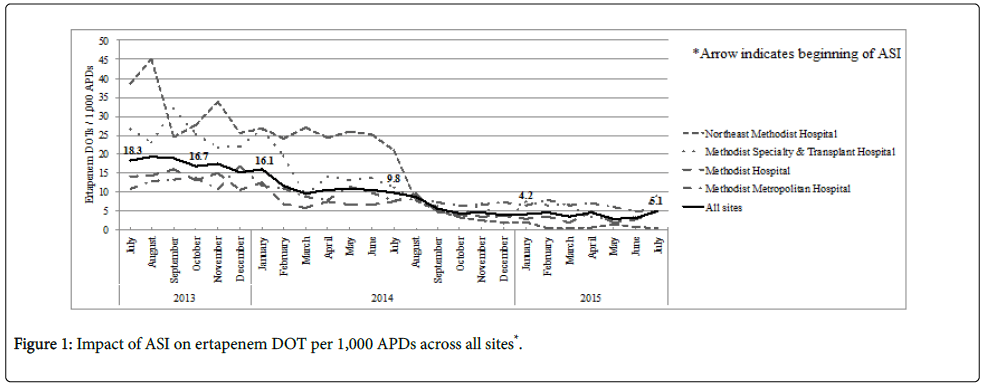
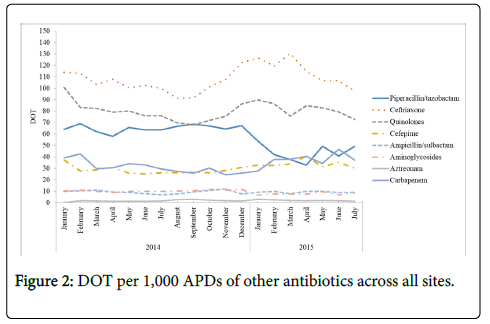
They were successful in significantly reducing ertapenem utilization by 60% with mean days of therapy (DOT) per 1000 adjusted patient days declining from 17.6 to 7.0, p<0.001. There was a decrease in overall antibiotic use but as expected, ceftriaxone and fluoroquinolones were highly utilized and increased around October 2014 (3 months after electronic alert restricting ertapenem). They reported stability of carbapenem use as a class. They only reviewed Pseudomonas aeruginosa, Escherichia coli and Klebsiella pneumoniae isolates; so potential effect on other Enterobacteriaceae could not be assessed. There was no change in % of P. aeruginosa non-susceptibility to carbapenems, however the average incidence of carbapenem non-susceptible P. aeruginosa isolates per 10,000 adjusted patient days decreased from 4.9 to 3.7 (p=0.03). There were no changes in % or average incidence of carbapenem non-susceptible E. coli or K. pneumoniae.
Copyright: © 2017 Delgado A, et al. Click to enlarge.
The authors achieved the goal of reduced ertapenem usage from 18.3 to 5.1 DOT, but did not show an associated change in carbapenem non-susceptible organisms. Furthermore, their overall carbapenem use was stable (though appears to have slightly trended upwards on the graph) despite significant ertapenem utilization reductions; without a breakdown of individual carbapenem use, it is impossible to know if there was a concordant increase in imipinem/meropenem use to account for this. Antibiotic shortages occurred during the study period, which unfortunately adds a confounder to the overall reduction of antibiotic utilization, as well as overall carbapenem utilization. – could these shortages have caused an increase in meropenem use? Additionally, limited (though number not specified) carbapenem non-susceptible isolates at baseline makes it difficult to draw conclusions about effect of the intervention on the antibiogram. However, it demonstrates well that a multifaceted intervention can have significant impact on antibiotic utilization.