Division of Infectious Diseases
UNMC Highlights Women in Science
As a medical student, I feel fortunate to be at UNMC, which values and supports women in medicine. One of the greatest examples of this empowerment championed is a program held this year called “UNMC’s Women in Science: Our Voices, Our Stories.” This event – sponsored by the McGoogan Library of Medicine, the Women’s Mentoring […]
Jul 29, 2019
Pharm2Exam Table: What is persistent MRSA bacteremia and how is it treated?
The following is a clinical review written by Ashleigh Grammar, PharmD, a recent graduate of the UNMC College of Pharmacy, and supervised by Scott Bergman PharmD FIDSA, Clinical Pharmacy Coordinator of Nebraska Medicine Antimicrobial Stewardship Program (@bergmanscott) What is persistent MRSA bacteremia and how is it treated? Methicillin-resistant Staphyloccous aureus (MRSA) (photo credit: CDC Public Health Image […]
Jul 22, 2019

Placing PICCs for Antibiotics – Potential Undue Risks May Outweight Benefits
PICC placement is common practice for intravenous (IV) antibiotic needs, however, we may be inadvertently placing certain patients at higher risks for complications. A recent study by Paje et al assessed the frequency of PICC placement among patients with CKD stage 3b or greater, a practice discordant with current guidelines. This prospective study included data […]
Jul 19, 2019

Dr. Susan Swindells to lead new TB prevention clinical trial
We are very proud to have Dr. Susan Swindells as a part of our division. A nationally and internationally renowned HIV clinical researcher, Dr. Swindells is a Professor of Internal Medicine-Infectious Diseases at University of Nebraska Medical Center. For many years she has led the Specialty Care Center in providing extraordinary care to patients with […]
Jul 15, 2019

A Message from Our ID Fellowship Leaders
Fellowship application season is nearing and as the leaders of our ID fellowship, we wanted to highlight some of the exciting aspects of our program. Our program and our division are growing. We began in 2011 with 2 fellows, grew to 4 in 2017, and are planning to expand to six fellows by 2021. We […]
Jul 11, 2019

EMET Student Profile – Samantha Cox, M1
Meet Samantha Cox, a new M1 student in our HIV Enhanced Medical Education Track! Tell us a little about yourself I moved to Omaha with my family from Saskatoon, Saskatchewan, when I was in elementary school and attended high school at Duchesne Academy. I completed my Bachelor’s degree in French and Biology at College of […]
Jul 9, 2019
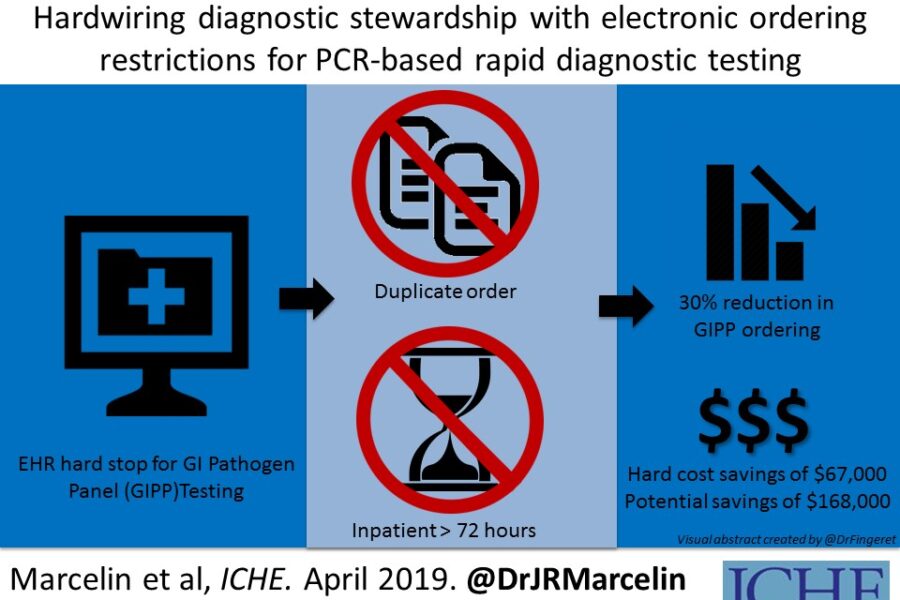
Inpatient Diarrheal Illness…Don’t Flush your Money: Save it with Diagnostic Stewardship!
Recently, a multidisciplinary team at UNMC published a diagnostic stewardship study in Infection Control & Hospital Epidemiology (ICHE) entitled: Hardwiring diagnostic stewardship using electronic ordering restrictions for gastrointestinal pathogen testing, that prompted a press release from The Society for Healthcare Epidemiology of America (SHEA), and a feature on an upcoming ICHE podcast episode. Drs. Jasmine Marcelin and Trevor Van […]
Jul 1, 2019
Everyone Should be Tested for HIV
Today is National HIV Testing Day, and one of the most fulfilling conversations to have with persons living with HIV (PLWH) is to share that since the 1980’s, we have made significant progress in the management of the AIDS epidemic. FDA approval of 27 antiretrovirals and 20 fixed dose combination antiretrovirals, increased HIV testing campaigns and […]
Jun 27, 2019
Propagation of Misinformation – Lessons From the 2019 Ebola Outbreak
This month, two concerning stories about the ongoing epidemic of Ebola virus disease (Ebola for short) in Africa grabbed our attention. On Monday, several social media sites circulated posts about Congolese refugees who had crossed the border from Mexico to Texas and tested positive for Ebola. The various posts circulated widely enough that they were […]
Jun 24, 2019

A Day in the Life of Central Venous Access Devices
This post comes courtesy of Dr. Mark Rupp, who recently published a study in the Journal of Infusion Nursing about outpatient maintenance practices for central venous access devices (CVADs)! Our patients are increasingly receiving intravenous therapy at home via indwelling CVADs. However, limited data exist regarding patients’ experiences with outpatient CVADs. Regina Nailon is the […]
Jun 18, 2019
Recent Comments